
By Dr. Ross Turchaninov
Phoenix, AZ
In the previous issue of JMS, in the ‘News From The Clinic’ section we published the clinical case “Medical Massage vs Pneumonia’s Residuals”:
https://www.scienceofmassage.com/2019/12/medical-massage-vs-pneumonias-residuals/
This case was sent to SOMI by our former student Curt Lezanic, LMT, CMMP who has developed a very successful Medical Massage practice in San Antonio, Texas. Besides helping patients with various somatic abnormalities, recently Curt started to branch out his practice by helping patients with different chronic visceral diseases which were referred to his clinic by local physicians.
Of course, Medical Massage can’t cure chronic visceral pathologies, but it can greatly help physicians treat and manage the intensity of symptoms and frequency of the flare ups. Medical Massage can do that by eliminating somatic components of the chronic visceral disorders which developed secondary as a reflex reaction of the soft tissues to the abnormal function of the affected inner organ.
While a majority of the therapists greatly enjoyed and learned from Curt’s publication and his clinical expertise, a significant number of therapists dismissed the publication with comments like “Fantasy” and even personally attacked its author with comments like: “Fallacy, “Misinformation” etc. These critics didn’t produce any supportive material and based their comments on ‘just because I said so.’ The material Curt shared with therapists was pure clinical observation and of course, didn’t required any references. That was the main foundation for the unjustified attacks.
These attacks illustrated a very unfortunate reality that some therapists don’t have even slightest idea how far they can go in helping patients when they know what to do, how to do it, and understand the importance of the place Medical Massage occupies in modern medicine. Therapists who continue to have such erroneous views not only undermine the clinical value of massage therapy they also dismiss Osteopathic Medicine in general since Medical Massage is an integral part of it.
Modern medicine since 1947 (Prof. Korr, 1947) clearly established scientific and clinical fact that inner organs and soft tissue, which share innervation within the same segments of the spinal cord, are in mutually productive reflex relations or in other words they are constantly talking with each other. These reflexes Medical Massage engages when it alters functions of the affected inner organ via soft tissue work. It is astonishing to observe that some therapists deny existence of the entire branch of medicine which is supposed to be ‘bread and butter’ of their profession!
Here are couple quotes from scientific publication where, in difference with some therapists, physicians expressed completely different opinions about clinical perspectives of MT application for the chronic visceral abnormalities:
From: Rehabilitation Medicine: Principles & Practice, 1999
“Massage stimulates cutaneous receptors and spindle receptors in the skeletal muscles. These produces impulses that reach the spinal cord which once there conceivably can produce myriad effects…. allowing for such a system, massage could have distant visceral effects”
Prof. J.J. Rechtein, DO, PhD, Prof. M. Andary, MD, T.G. Holmes, MD, Prof. J.M. Wieting, DO
From: Physical Medicine & Rehabilitation, 2005
“All somatic and visceral tissues can be negatively affected if they are innervated by the nerves from a spinal segment that receives afferent information from an area of somatic dysfunction. If this is true, then it follows that alleviation of somatic dysfunction via massage results in optimized function of the somatic and visceral system that are innervated by the same spinal segment”
Prof. J.W. Atchinson, DO, S.T. Stoll, PhD, W.G. Gilliar, DO
I would like to finish this introductory part with quotes from two great scientists, physicians and authorities in clinical application of massage therapy, Dr. J. Weiss, MD from USA and Professor Aksenova, MD from Russia:
“The reflex value of massage is probably the most important of all. From this point of view we may retain a conventional estimate of the merits of massage.’
Dr. J. Weiss, MD (1952), USA
“The treatment of any chronic disorder of the human body has to include the appropriate method of massage therapy.’
Prof. A.M Aksenova, MD (1998), Russia
Therefore, we decided to publish a follow up post which illustrates the successful impact of MM therapy in even more complex clinical cases than Curt’s and provide requested reference material.
In our clinic in Phoenix we regularly work with patients who suffer from various chronic visceral abnormalities and we observe similar results as was reported by Curt in his publication. To support Curt’s clinical case we have chosen a patient from our clinic who suffered from Chronic Emphysema.
CLINICAL HISTORY
The 82 year-old male was successfully treated in our clinic for different somatic problems: Chronic Lower Back Pain, Rotator Cuff Pain as well as neurological syndromes: Sciatica and Benign Paroxysmal Positioning Vertigo. All these abnormalities were eliminated, and he was seen only for supporting sessions since the patient is dedicated golfer.
Several months ago, it was obvious that the patient started to breathe heavier that he usually did, and we suggested that he didn’t waste time and go to see his pulmonologist asap.
The clinical history of this patient is very complex, especially regarding his pulmonary function. In 1991 he was diagnosed with left side breast cancer and went through a total mastectomy with lymph nodes removal, long chemotherapy and radiation therapy. As a result of radiation, the soft tissues on his left chest developed moderate fibrosis which compromised his respiratory function and every 6 months his pulmonary function was examined by pulmonologist.
For years he was regularly checked for possible cancer activity and with proper medications he became cancer free. However, in 2015 his CPA started to claim up and a newly developed cancer spot was detected in his left lung. The cancer therapy immediately started and besides adjusting the medication he was treated with gamma-knife.
Gamm-knife allows oncologists to deliver radiation precisely to the affected part of the lung. However, to do that correctly the markers must be inserted into the lung around the newly discovered spot first, to guide the radiologist. While he was getting therapy, his left lung collapsed creating condition called pneumothorax. After lung restoration his breathing never fully recovered and became additionally compromised. To keep airways potent, he was prescribed to use an inhaler which assisted him with breathing.
As we suggested, the patient went to his pulmonologist and after running necessary tests the doctor registered a significant drop in pulmonary function and diagnosed him with Chronic Emphysema. In average his blood oxygenation was 93-94% at rest.
These numbers indicate significant decrease in pulmonary function and the pulmonologist suggested to switch to a more patent inhaler with steroids to keep the patient’s airways open. However, the patient’s oncologist wasn’t happy with such a plan since prolonged and regular usage of steroid inhalers is going to suppress the patient’s immune system which at this point the important job to do was to control the cancer. Since our clinic helped the patient with a variety of somatic and neurological problems he asked if anything could be done to help him with improvement of his pulmonary function.
EVALUATION
Breathing Pattern
Visual observation of the patient’s breathing illustrated that its normal pattern is profoundly disturbed. Normally during quiet respiration most of the gas exchange happens in the lower and middle portions of the lungs. We actively engage upper parts of the lungs only when extra oxygen is needed, for example, during physical exercises.
Also, during quiet breathing, the inhalation is an active process when we use our respiratory muscles to expand the thoracic cage and in combination with a descending diaphragm level of oxygen in the blood is maintained. To the contrary, the exhalation, during quiet breathing, is a passive process since the thoracic cage simply collapses when we release tension in the respiratory muscles needed for the chest expansion during inhalations.
The video below illustrates the breathing pattern of our patient during forced inhalations. Please notice that during each inhalation the patient elevates his shoulders rather than expanding his middle and lower chest.

Also, when he walks even one flight of stairs, he greatly increases inhalation efforts and also starts to actively exhale air like he is doing intense exercise.
Measurement of his chest expansion seeing in the video below conducted independently by one of our physicians showed minimal chest expansion during each deep inhalation.

Chest and Soft Tissues
Examination of the patient’s intercostal spaces indicated that during deep inhalation there is very limited rib expansion. Fig. 1 illustrates placement of the thumb into the 6th intercostal space during the peak of inhalation. As you can see, it is very difficult to place the thumb between two neighboring ribs at the peak of inhalation because the ribs are not driven apart.

Fig. 1. Intercostal space before the MM therapy
Reflex Zones
Evaluation of the soft tissues indicated the following pattern of reflex abnormalities according to Glezer/Dalicho Zones (see Fig. 2).
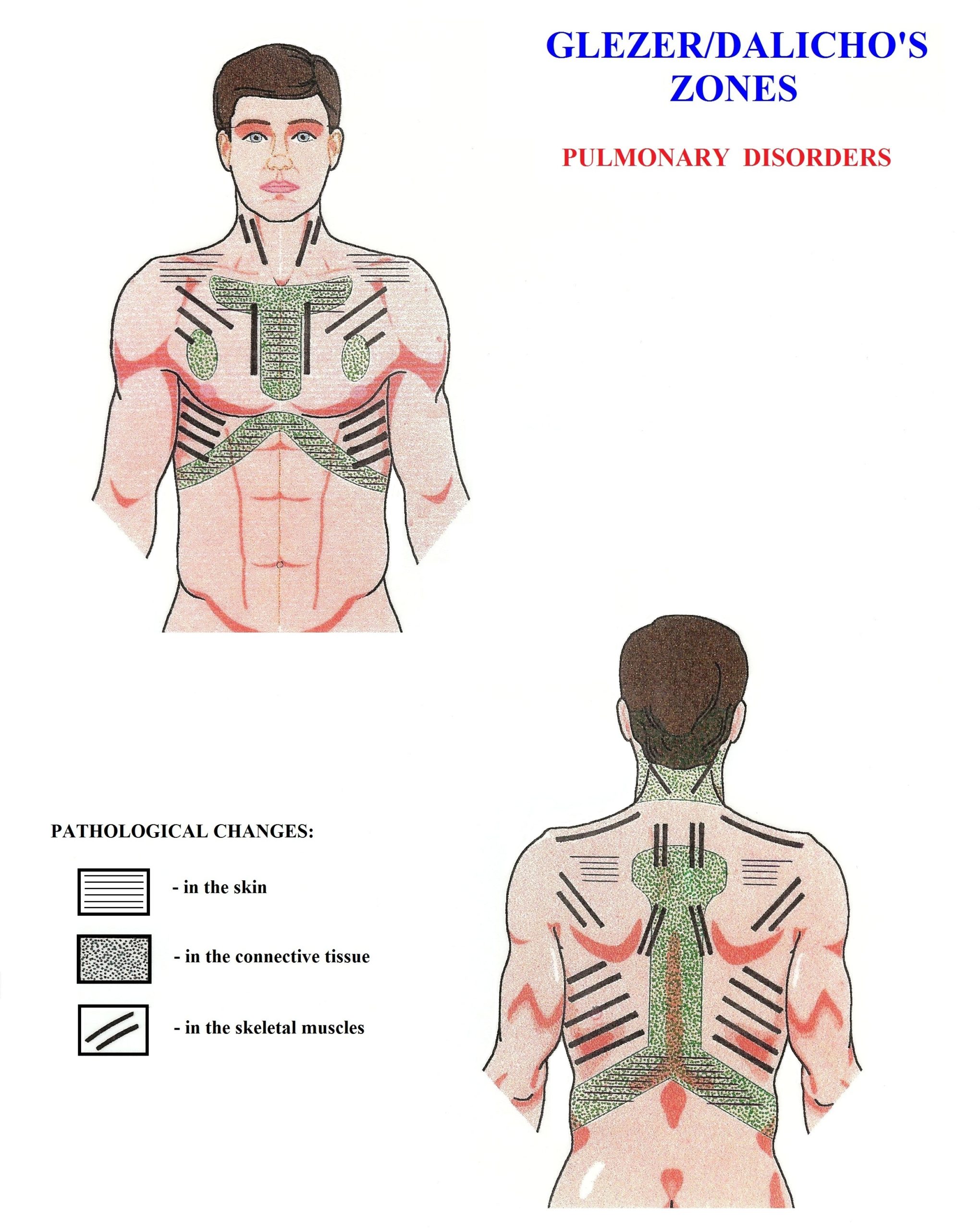
Fig. 2. Glezer/Dalicho Zones in cases of Chronic Pulmonary Disorders (Glezer and Dalicho, 1955)
1. Cutaneous Reflex Zones (CTRZ)
Sensory Test indicated presence of CTRZ in the left parasternal area and above left scapula Areas with black horizontal lines in Fig. 2.
2. Connective Tissue Zones (CTZs)
Tension in the first level of CTZs (in the dermis of the skin) was detected using the first part of Kibler’s Technique (Kibler, 1953) along the parasternal area and along the lower part of the rib cage on the left.
Tension in the third level of CTZs was detected in the middle back between T4 and T12 using Opposite Shift Technique. It reflected increased tension in deep fascia which separated the trapezius from the rhomboids and paravertebrals. These areas indicated in Fig. 2 by green dots
3. Reflex Zones in the Skeletal Muscles
Multiple locations of the active TP were recorded in the anterior scalene muscle, pectoralis major and minor, upper and lower trapezius muscle, rhomboids and intercostals.
4. Reflex Zones in the Periosteum
Active reflex zones were recorded along the occipital ridge, medial edge of the left scapula, lateral surfaces of the spinous processes especially in the T5-T9 thoracic vertebrae; along edges of the same ribs and finally along the entire left lateral side of the breastbone. In all these areas even slight application of pressure triggered acute pain.
TREATMENT
The patient exhibited a very complex clinical picture which included profound local and reflex changes in the function of the entire thoracic cage. The mobility of the chest must be restored to help respiratory muscles to work more efficiently while secondarily reflex zones must be eliminated to help in reducing bronchoconstriction.
In 2013 JMS published a two-part article, ‘Medical Massage For The Treatment Of Patients With Pneumonia’ which was contributed to our publication by Russian physician and scientist Dr. T.V. Mitichkina. This article was excerpted from Dr. Mitichkiva’s textbook published in 2012. This textbook was written for pulmonologists to teach doctors how to prescribe Medical Massage Therapy and control its correct execution by massage therapists. Currently this textbook is widely used in the Russian Federation as a main scientific and clinical source in continuing education classes for pulmonologists.
For everyone who would like to read the theoretical aspects on how Medical Massage Therapy is able to help patients with chronic visceral abnormalities, please read the first part of Dr. Mitichkina’s article:
https://www.scienceofmassage.com/2013/01/medical-massage-in-cases-of-pneumonia-part-i/
To go over the Medical Massage protocol in case of pneumonia and other chronic pulmonary disorders please read Part II of the article:
We used the Medical Massage protocol presented in Part II of Dr. Mitichkina’s article as a framework for the treatment of our patient with some additions which are needed regarding its application in cases of Chronic Emphysema: wave kneading of the abdominal muscles, enforcement of abdominal breathing, relaxation of the torso non-respiratory muscles, decompression of fascia and percussion along intercostal muscles within spaces and along costal edges of two neighboring ribs.
RESULTS
As a result of conducting Medical Massage therapy within a 3 week span of 2-3 weekly Medical Massage sessions, all reflex zones were eliminated one by one. We started with skin and fascia and finally got rid of hypertonic abnormalities (active trigger points and hypertonuses) in respiratory muscles and secondarily changes in the periosteum of the thoracic cage and neck.
Video below illustrates the restoration of the normal breathing pattern after course of MM therapy. Now the patient is able to expand lower parts of the chest and restore blood oxygenation instead of shoulders elevation which contributes less to the overall oxygenation process.

Fig. 3 below illustrates the rib mobility before and after the course of Medical Massage Therapy. You may observe how deeper the thumb’s placement is between two neighboring ribs at the peak of inhalation. Deeper submergence of the thumb between two ribs seen in the Fig. 3b indicates that lower and middle ribs are now actively moving during chest expansion while the patient inhales even quietly.
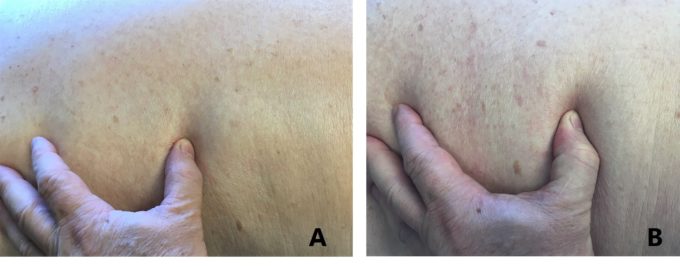
Fig. 3. Active ribs movement before and after Medical Massage Therapy at the peak of inhalation
The video below illustrates measurement of the chest expansion conducted by an independent family physician after the course of Medical Massage therapy. The overall chest’s expansion increased by one inch as a result of restoration of ribs mobility and soft tissues elasticity. This is huge improvement for this patient since it will dramatically decrease intrapleural pressure, assistance in the descending of diaphragm and increase gas exchange in the middle and lower parts of the lungs where the majority of oxygenation is supposed to happen.

Finally, Fig. 4 illustrates the patient’s blood oxygenation at rest measured in our clinic before Medical Massage therapy started and at the end of it. 98% is normal for the resting state and age of our patient. Please remember that what separates numbers in both pictures is course, of Medical Massage Therapy!

Fig. 4. Blood Oxygenation measured by oximeter before and after MM therapy
LESSONS:
1. Therapists who regularly work on clients and patients frequently are the first who may observe even small changes in their walking, breathing, color of the soft tissues etc. That’s why it is so important to pay attention to all even small fluctuations in the patient’s appearance or behavior.
2. In the majority of somatic cases the Medical Massage Therapy by itself can be ultimate solution to the pain and dysfunction. However, in cases of chronic visceral abnormalities the Medical Massage is just another tool (in addition to medications, injections, diet etc.) physicians must use to help patients.
3. Every chronic visceral disorder carries a somatic component and there are not any other health practitioners in medicine except the MM therapists who have tools, and time to detect and decisively eliminate reflex zones in the soft tissues which formed secondarily as a CNS reaction to the inner organ dysfunctions.
REFERENCES
Aksenova, A.M., Romanova, M.M. Reflex Massage in Cases of Gastro-Intestinal Disorders. Vopr. Kurortol Fiziother. Lech. Fiz. Kult. 6, 24-26, 1998
Atchinson J.W., Stoll, S.T., Gilliar, W.G. Manipulation Traction & Massage. In: Physical Medicine &Rehabilitation. Edited by: Dr. R.L. Braddon, “W.B. Sandesr Co’, Philadelphia, 2005
Glezer, O., Dalicho, V.A. Segmentmassage, Leipzig, 1955
Kibler, M. Segment-Threapie. Stuttgard, 1953
Korr, I.M. The Neural Basis of the Osteopathic Lesions. JAOA, Nov. 47(4):191-198, 1947
Mitichkina T.V. Rehabilitation of Patients with Pneumonia. Novokuznetsk Medical University, Novokuznetsk, 2012
Rechtein, J.J, Andary, M., Holmes, T.G., Wieting, J.M. Rehabilitation Medicine: Principles & Practice, “Lippincott-Raven”, Philadelphia, 1999
Weiss J. Effect of Massage on Muscle Temperature and Radiosodium Clearance. Arch Phys. Med., July:399-405, 1952
Category: Blog
