
The patient/client evaluation consists of three equally important steps that contribute valuable data to the correct assessment of the tissues and designing an optimal treatment strategy. Therefore, an essential part of our Medical Massage training is dedicated to: visual observation, clinical interview, and finally, palpation and testing. This post addresses the importance of visual observation and tries to emphasize its clinical value for therapists.
Thank you to everyone who shared their opinions. It is excellent that we all can exchange data and ideas online. Let us summarize the posted answers and some of them are partially correct:
1. Edema
Yes, edema is present in both cases, but it is not the initial trigger but rather the consequence of it.
2. Tension in IT band
The visual signs of tension in IT band are going to be seen on the lateral aspect of the knee.
3. Osteoarthritis
Indeed, both patients are suffering from OA, but visual observation of both knees points to another pathology that, by the way, may accompany OA
4. Venous insufficiency
In cases of venous insufficiency, the edema will not have a local character but will be widespread.
5. Scar tissue
The scar tissue won’t produce localized edema seeing in the medial aspects of both knees.
6. Total knee replacement
As you may read below, the total knee replacement may trigger similar changes in the operated knee, but the question was about visual changes in the knee itself before any surgery.
7. Postural changes (tilted pelvis, instability of the knee, etc.) and altered gait (Plantar Fasciitis, Achillodynia, etc.)
Postural changes, as well as altered gate, may trigger this abnormality, but the question was about the visual observation of the knee itself.
8. Obesity
Yes, obesity can be an aggravating factor, and it is present in both patients, but it doesn’t explain the nature of knee changes on the local level.
9. Rheumatoid arthritis
The acute flare-up of RA will affect the entire joint (the joint is swollen and red), especially along the joint’s line.
10. Refer to the physician
This suggestion is incorrect for those who practice clinical aspects of MT. This pathological condition is solely in massage therapists’ hands and a scoop of practice. No medications, injections, or exercises can deliver stable clinical results even closely compatible with Medical Massage therapy.
The correct answer to posted pictures:
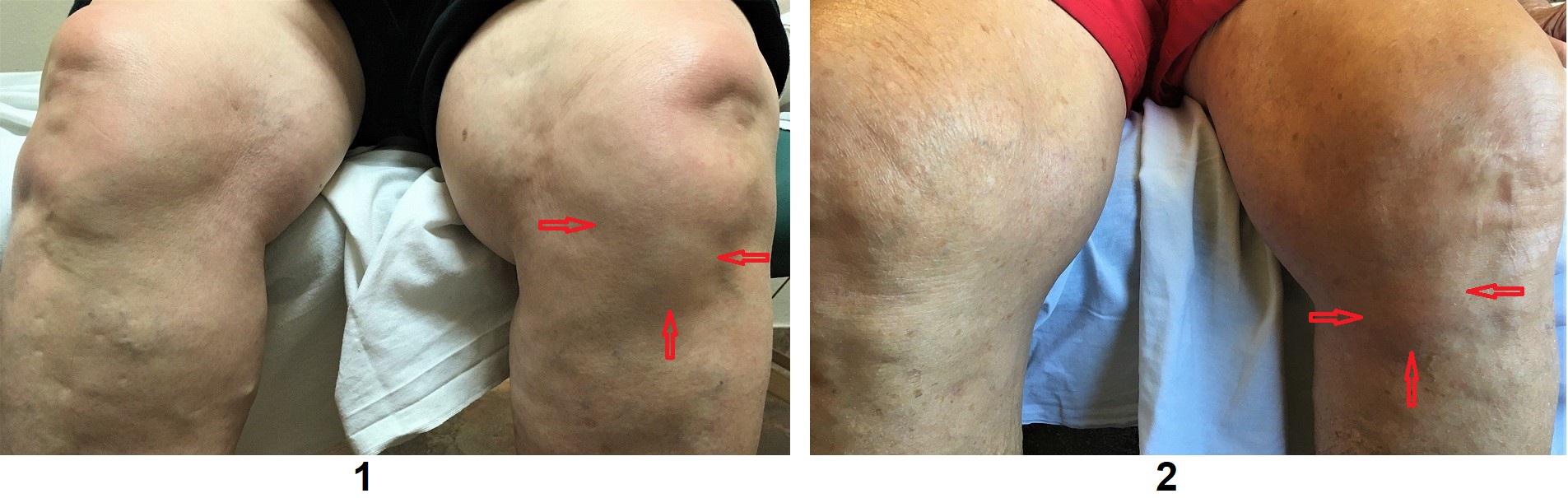
Both patients from our clinic suffered from Goosefoot (or ‘pes anserine‘) Tendinitis, which is responsible for anterior and/or medial knee pain. Those therapists who answered bursitis were correct.
Goosefoot Tendinitis is the local swelling of tendons of the sartorius, gracilis, and semitendinosus muscles at their insertion into the anterior/medial aspect of the tibial tuberosity with or without simultaneous inflammation of underlying bursa there. Red arrows indicate both areas where visual observation of local edema suggests the possible presence of Goosefoot Tendinitis. Please compare to the opposite side.
The patient in the first picture had acute Goosefoot Tendinitis AND bursitis (the area is more swollen, and the skin even has visual redness). In contrast, the patient in the second picture had only Goosefoot Tendinitis (the tissue on the anterior/medial knee is less swollen).
Of course, the presence of Goosefoot Tendinitis/bursitis should be confirmed by local palpation of the anterior/medial aspect of the tibial tuberosity. This post addresses ONLY the clinical value of visual observation, which frequently gives the first an important clue. A further detailed evaluation is always required.
With the rise of widespread knee replacement surgery, we began to see more and more patients with inflamed ‘goosefoot’ in our clinic. Most often, knee replacement surgeries were performed without complications and with stable and functional artificial knee (i.e., knee endoprosthesis); however, patients continued to suffer from anterior knee pain. Two of our patients underwent a second unnecessary surgery to implant a smaller endoprosthesis. As it turned out, the real cause of their knee pain was Goosefoot Tendinitis caused by tendon friction against the medial aspect of the endoprosthesis and periostitis of the tibia formed along its contact with the endoprosthesis.
Of course, the other causes of anterior knee pain must be ruled out first. For example: Femoral Nerve Neuralgia, a flare-up of Osteoarthritis, instability of medial collateral ligament, damage of tibial tuberosity, tendinitis of the patellar ligament, etc.
Our patient from the first picture developed Goosefoot Tendinitis and Bursitis after she fell on her knee, while the patient from the second picture developed Goosefoot Tendinitis due to the altered gate as a result of a long history of chronic lower back pain. In both scenarios, the local treatment to eliminate Goosefoot Tendinitis must be used.
The correct Medical Massage protocol for Goosefoot Tendinitis helps quickly eliminate this frequently missed cause of anterior knee pain. The therapy is simple: drain the inflamed area, decompress the fascia, address the sartorius, gracilis, and semitendinosus muscles separately (decompress the muscles with correctly applied kneading techniques, eliminate active and sleeping trigger points and restore the anatomical length of all three muscles using Muscle Energy Techniques), address the inflamed tendons, and finally, address the periosteal trigger points at the tendons’ insertions.
Conclusion: in cases of local swollenness on the anterior/medial surface of the tibial tuberosity and pain in the anterior and/or medial knee, please consider Goosefoot Tendinitis for future more detailed palpatory evaluation.
Join us for Medical Massage Seminars in Chicago, October 1-3. Don’t miss the opportunity to learn Medical Massage based on the science of its clinical application. For further details, please click the link here:
Category: Blog